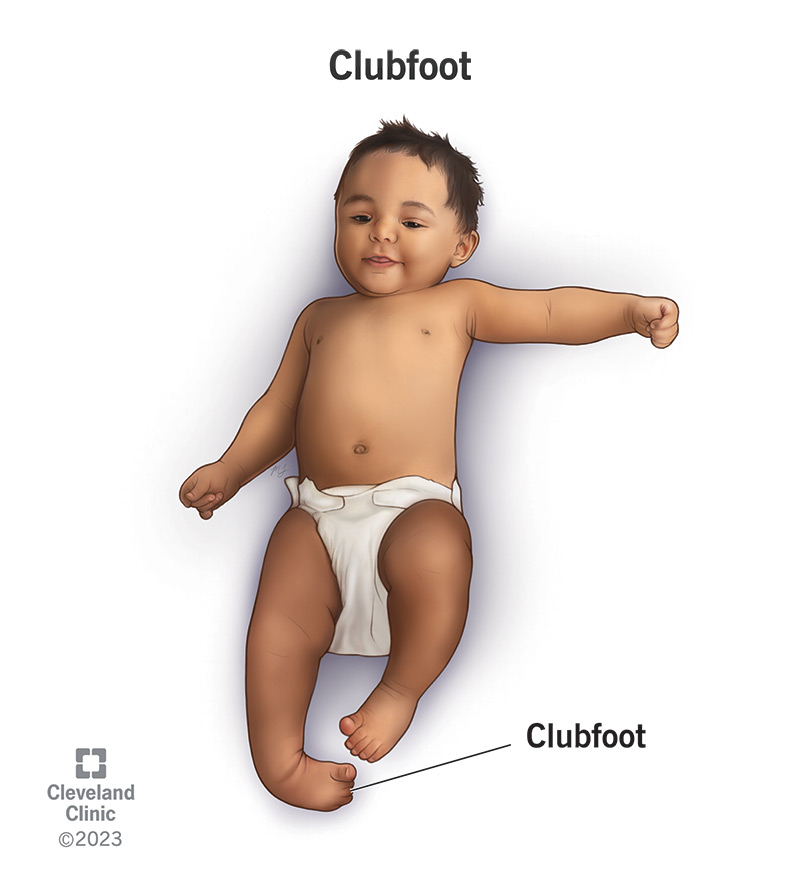
The treatment should begin in the first few weeks of life. The deformities should be treated step by step firstly adduction, then inversion and then equinus.
Techniques used by the physiotherapist
- Ponseti’s technique.
- Rhythmic and repeated gentle manipulation.
- Gentle stretching.
- Strapping and Plaster of Paris (POP).
Ponseti’s technique: The foot is supinated to align it and the calcaneus with the navicular. This supination is maintained as the talonavicular position is improved by abduction toward and then beyond the neutral plane. It is Ponseti’s recognition of medial foot column plantar flexion and the need to invert the entire foot to align all metatarsals in the same plane in the initial phase of manipulation differentiates his method of manipulation from others. Once adduction and inversion have been corrected, however, percutaneous Achilles tenotomy is done to correct equinus if it does not respond quickly to serial manipulation into dorsiflexion rather than the much more prolonged stretching with repetitive casts and wedging is done. Once the foot has been corrected, great emphasis is placed on maintaining the correction with full-time bracing for 3 months and nighttime bracing for 2–4 yrs Well-molded long leg casts are applied every 4–7 days. The short leg cast is applied first from toes to just below the knee and this is then converted to a long leg cast to upper-thigh with the knee flexed to a right ankle and the leg externally rotated to correct tibial torsion.
To correct the varus deformity: The affected side knee is placed at 90o flexion to prevent damage to the lower end of tibial and fibular epiphyses, and the knee joint. Then the soft tissues of the right foot is passively stretched, the forefoot is flattened. Thus correcting the adduction. Then the foot is turned such that the sole is faced outward i.e eversion, thus correcting the inverted foot. The strectch is given for 2 minutes and repeated five times.
To correct the equinus (plantar flexion deformity): The heel is cupped with the right hand from the front of the foot and upward pressure is applied to it bringing the forefoot upward. This brings the ankle into dorsiflexion. Each manipulation lasts for about two minutes and the entire procedure is repeated five times.
Strapping: To maintain the feet in the corrected position, strapping is done. One therapist can stabilize the baby’s limb and the other can carry out the procedure. Strapping begins by holding the manipulated right foot to the overcorrected position. The first strip is applied from the medial border of the midpoint of the right leg down under the ipsilateral heel then along the lateral border of the leg to the lower 1/3 of the thigh with the knee flexed at 90o. This is to correct the heel varus deformity by eversion of the foot.
The second strip is applied over the dorsum of the mid-foot from lateral to medial then under the sole back to the lateral border of the mid-foot then along the border of the leg over the lower 1/3 of the thigh with the knee still at 90o. This is important to correct the equinus deformity abduction of the forefoot.
To bring the ankle into dorsiflexed position, the third strip is applied over the dorsum of the forefoot from lateral to medial, then along the plantar surface of the forefoot to the lateral border of the leg over the lower 1/3 of the thigh. The last strip is applied circumferentially around the leg at a point 2cm above the ankle joint. This is to correct the bowstring appearance of the lower 1/3 of the leg, the ankle, and the foot, and to increase eversion. At the end of the procedure, the therapist can wait and observe the limb for 30 minutes to check for any compromise to circulation. A layer of cotton wool (the rolled type in layers), enough to cover the malleoli was applied at medial and lateral malleoli of both ankles to avert pressure sore; Where the strips of the straps were circumferentially applied, in-between spaces were avoided to prevent window oedema. The strips of the straps should be smoothly applied and no wrinkles are permitted, to prevent skin excoriation. For the first six weeks, the baby is seen thrice a week and strapping applied twice per week. From the period the baby is 7 to 12 weeks, the strapping is done once per week.
Plaster of Paris: At three months improvement will be seen. Baby at third month by this period (that is when the baby is three months), the strapping is no more effective because he can kick vigorously with the lower limbs. It was then replaced with a full leg plaster of Paris (POP) with the knees at 90o of flexion. The plaster was changed weekly for the first eight weeks of application and the knees and feet mobilized on each occasion. Thereafter it was applied and changed forth-nightly for another eight weeks. The plaster was finally removed when the baby was exactly seven months. At eight months and three weeks, he started standing with support and a good plantigrade position. At the thirteenth month, the baby can walk.